Carrier Frequency: Hardy-Weinberg & the 2pq Step
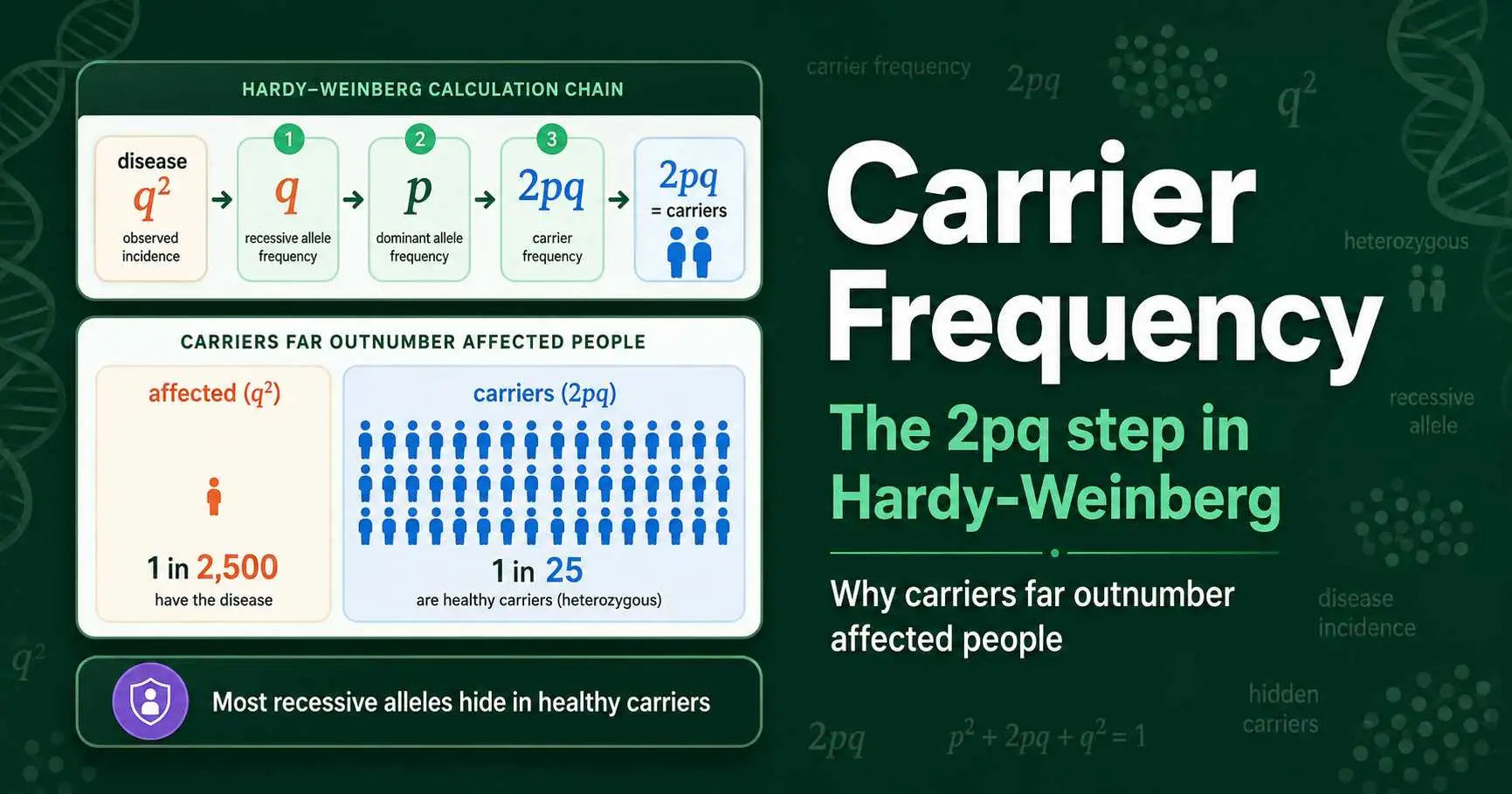
To find the carrier frequency of a recessive condition with Hardy-Weinberg, you calculate 2pq, the frequency of heterozygotes. Start from the disease incidence, which equals q², take its square root to find q, use p + q = 1 to find p, then multiply 2 times p times q. For a condition affecting 1 in 10,000 people, q² is 0.0001, so q is 0.01, p is about 0.99, and the carrier frequency 2pq is roughly 0.0198, meaning about 1 in 50 people carry the allele. Carriers almost always vastly outnumber affected individuals.
Carrier frequency is one of the most practically important quantities in all of genetics, because carriers are invisible in clinical data yet carry and transmit recessive disease alleles, often without any idea that they do. Hardy-Weinberg is the tool that reveals them. This guide explains the 2pq step in detail, shows why carriers so dramatically outnumber affected people, and works through real examples for cystic fibrosis, PKU, and sickle cell. The carrier calculation can be run with a calculator, but understanding the 2pq logic is what makes the numbers meaningful.
What a Carrier Is and Why They Are Hidden
A carrier is an individual who has one copy of a recessive allele but does not show the associated trait or condition in any way. In genetic terms, a carrier is precisely a heterozygote, with one normal allele and one recessive allele, giving the genotype Aa. The single normal allele is enough to produce a healthy phenotype, so the carrier appears completely unaffected.
This is exactly what makes carriers so important and so difficult to detect. Because they look identical to individuals with two normal alleles, you cannot identify carriers by observation. In a population, the homozygous dominant individuals (AA) and the heterozygous carriers (Aa) share the same phenotype, blending together. Only the homozygous recessive individuals (aa), who actually show the condition, stand out. The carriers are hidden in plain sight, silently carrying a disease allele they can pass to their children.
The practical importance is enormous. Two healthy carriers who have children together face a real chance of an affected child, even though neither parent shows any sign of the condition. This is the classic situation behind many inherited diseases, and it is why estimating how many carriers exist in a population is a central task in genetics and medicine. Since you cannot count carriers directly, you need a mathematical way to estimate them, and that is precisely what Hardy-Weinberg provides. The difference between carriers and affected individuals rests on the distinction between a heterozygote, with one copy of the allele, and a homozygote, with two, which the 2pq and q² terms capture.
The 2pq Step: Calculating Carrier Frequency
The carrier frequency in a population is given by 2pq, the heterozygous term of the Hardy-Weinberg equation. This single expression is the key to estimating how many people silently carry a recessive allele, and learning to calculate it is the heart of this topic.
The procedure starts, as always, from what you can observe. The frequency of affected individuals, the disease incidence, equals q², because affected people are homozygous recessive. From q² you take the square root to find q, the recessive allele frequency. Then p + q = 1 gives you p, the normal allele frequency. Finally, you multiply 2 times p times q to get the carrier frequency. The full chain is: disease incidence gives q², square root gives q, subtract from 1 gives p, and 2pq gives the carriers.
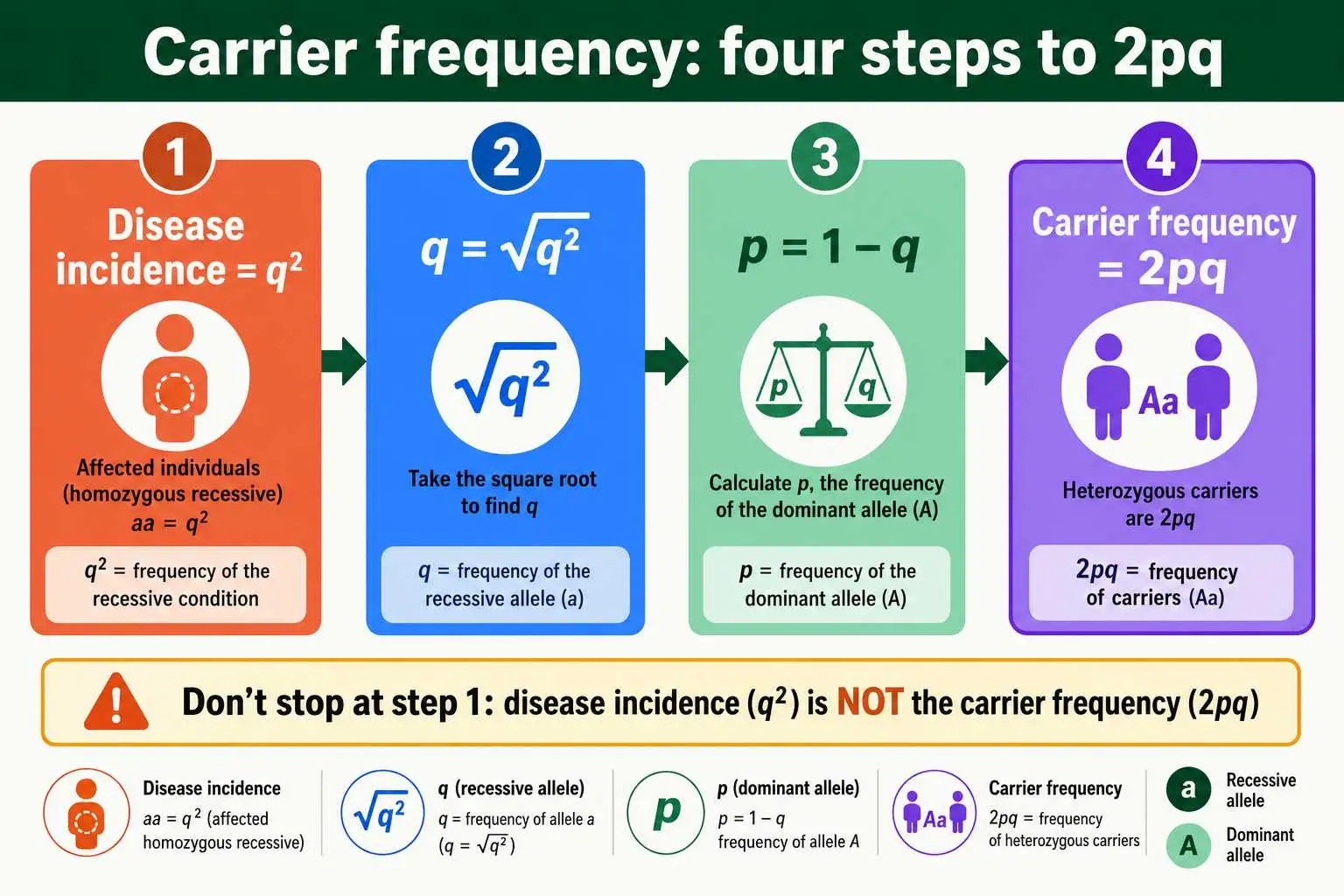
Writing these four steps down before starting any carrier problem keeps the workflow clear. The most common mistake is stopping too early, reporting the disease incidence itself as the carrier frequency. The disease incidence is q², not 2pq, and these are very different numbers. Someone who sees "1 percent of people have the condition" and answers that 1 percent are carriers has confused q² with 2pq and stopped two algebra steps short. The carrier frequency is almost always far larger than the disease incidence, which the worked examples will make vivid. The detailed mechanics of each step are covered in our guide on using the Hardy-Weinberg equation, but for carrier problems the destination is always 2pq.
Why Carriers Outnumber Affected Individuals
The most striking and important lesson about carrier frequency is that carriers vastly outnumber affected individuals, especially for rare conditions. This is not a quirk of particular diseases; it is a mathematical consequence of the Hardy-Weinberg relationship, and it has profound public health implications.
The reason lies in comparing 2pq with q². When the recessive allele is rare, q is small and p is close to 1. The affected frequency, q², involves squaring a small number, which makes it very small indeed. The carrier frequency, 2pq, is roughly 2q when p is near 1, which is much larger than q². For example, if q is 0.01, then q² is 0.0001 while 2pq is about 0.02, making carriers two hundred times more common than affected individuals. The rarer the condition, the more extreme this ratio becomes.
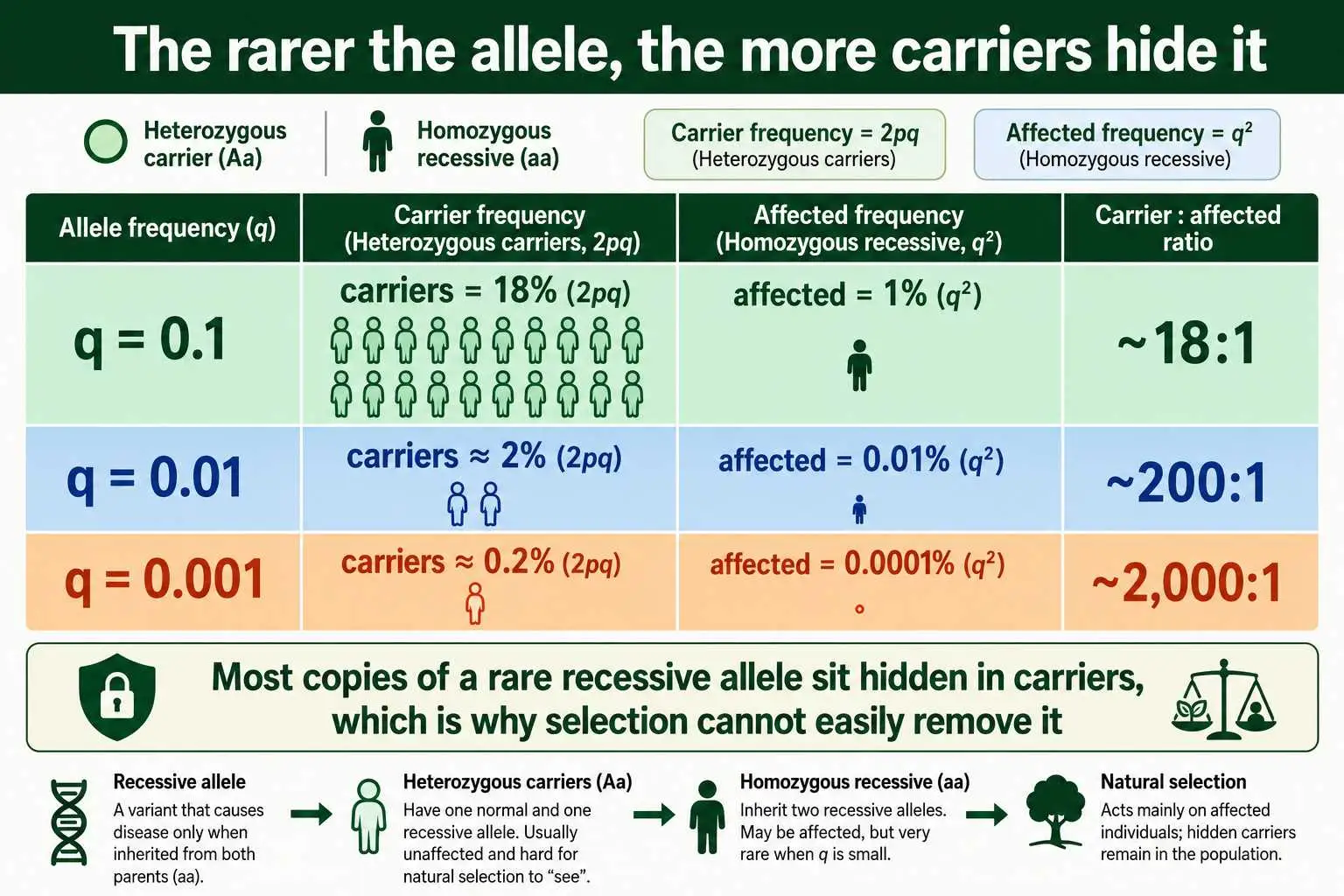
This explains a deep puzzle: why do recessive disease alleles persist in populations rather than being eliminated by natural selection? The answer is that the vast majority of disease alleles are hidden in healthy carriers, not exposed in affected individuals. Selection can only act on the phenotype it can see, the affected homozygotes, but most copies of the allele are shielded inside carriers where selection cannot reach them. So the allele persists across generations, surfacing as an affected individual only when two carriers happen to have children together. This insight, that rare recessive alleles live mostly in carriers, is one of the most important practical takeaways from population genetics.
The scaling is worth dwelling on because it is so counterintuitive. As a recessive allele becomes rarer, the ratio of carriers to affected individuals grows without bound. At an allele frequency of 0.1, carriers outnumber affected people roughly 18 to 1. At a frequency of 0.01, the ratio is about 200 to 1. At 0.001, it climbs to roughly 2,000 to 1. As one genetics teaching resource explains, this is why the carrier frequency and the disease incidence are never the same number, and why reporting the disease rate as if it were the carrier rate is such a common and serious error. The rarer the condition, the more dramatically the hidden carriers outnumber the visible cases.
Worked Example: Cystic Fibrosis
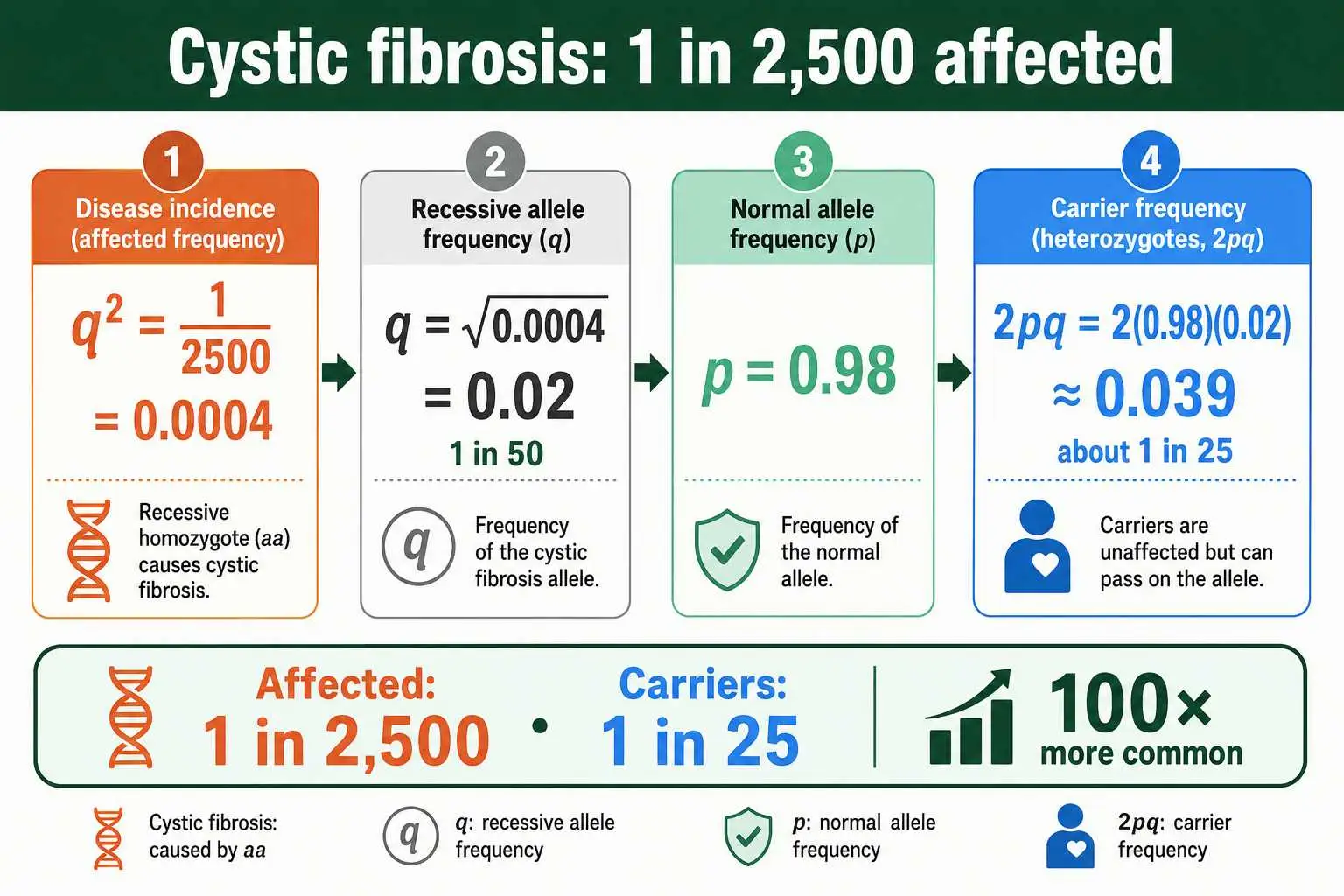
Cystic fibrosis is the textbook example of carrier frequency, because it is a relatively common recessive disorder with well-documented incidence. In northern European populations, cystic fibrosis affects roughly 1 in 2,500 newborns. Let us find the carrier frequency.
Start with the disease incidence. Affected individuals are homozygous recessive, so q² equals 1 in 2,500, which is 0.0004. Take the square root to find q, which is the square root of 0.0004, giving 0.02, or 1 in 50. Since p + q = 1, p equals 0.98, very close to 1. Now calculate the carrier frequency, 2pq, which is 2 times 0.98 times 0.02, giving approximately 0.0392, or about 1 in 25.
The result is remarkable. While only 1 in 2,500 people is affected by cystic fibrosis, roughly 1 in 25 people is a carrier, which is one hundred times more common.
This means that in a population, carriers of the cystic fibrosis allele are everywhere, even though the disease itself is relatively uncommon. This is exactly the information genetic counselors and screening programs need, because the chance of two carriers having children together, and thus of an affected child, depends on how common carriers are. The cystic fibrosis numbers show why carrier screening is so valuable: many people carry the allele without any family history or symptoms to warn them.
More Examples: PKU, Tay-Sachs, and Sickle Cell
Several other recessive conditions illustrate the same carrier-frequency logic, each with instructive numbers. Working through a few builds intuition for how the math plays out across different incidence rates.
Phenylketonuria, or PKU, affects about 1 in 10,000 babies. So q² is 0.0001, q is 0.01, and p is about 0.99. The carrier frequency 2pq is 2 times 0.99 times 0.01, which is about 0.0198, or roughly 1 in 50. Again carriers, at 1 in 50, far outnumber affected individuals at 1 in 10,000, by a factor of two hundred. Tay-Sachs disease in the Ashkenazi Jewish population has an incidence of about 1 in 400, so q² is 0.0025, q is 0.05, and the carrier frequency works out to about 1 in 10, a notably high carrier rate that reflects the elevated allele frequency in that population.
Sickle cell anemia provides a contrasting example where the allele is far from rare in certain populations. In some regions, the affected frequency can be as high as 9 percent, so q² is 0.09, q is 0.3, and p is 0.7. The carrier frequency 2pq is 2 times 0.7 times 0.3, which is 0.42, meaning a striking 42 percent of the population carries one copy of the sickle cell allele. This unusually high carrier frequency reflects the heterozygote advantage that sickle cell carriers have against malaria, a topic explored in our guide to genetic disorders and Punnett squares. Across all these examples, the pattern holds: carriers outnumber affected individuals, and the rarer the disease, the wider the gap.
A Useful Shortcut for Rare Alleles
For rare recessive conditions, there is a handy shortcut that simplifies the carrier calculation. When the disease allele is rare, the frequency of the normal allele p is very close to 1, which lets you approximate the carrier frequency more simply.
Because p is approximately 1 for a rare allele, the carrier frequency 2pq is approximately 2q. And since q is the square root of the disease incidence, the carrier frequency is roughly twice the square root of the disease incidence. This gives a quick way to estimate carriers: take the square root of the disease frequency and double it. For a condition affecting 1 in 10,000, the square root of 0.0001 is 0.01, and doubling gives 0.02, or 1 in 50, matching the full calculation closely.
This approximation is widely used in genetics and medicine because it is fast and accurate enough for rare alleles. The small error from treating p as exactly 1 is negligible when q is tiny. The shortcut also reinforces the key relationship: carrier frequency is roughly double the square root of disease incidence, which makes the dramatic difference between carriers and affected individuals immediately visible. For a disease affecting 1 in a million, the square root is 1 in 1,000, so carriers are about 1 in 500, two thousand times more common than affected individuals. The shortcut makes this scaling easy to see at a glance, and it is the version most often used in clinical and exam settings, where speed matters and the disease allele is genuinely rare enough for the approximation to hold.
Limitations of the Carrier Frequency Estimate
The Hardy-Weinberg carrier estimate is powerful, but it rests on assumptions that real populations do not always meet, so it is important to understand when the estimate may be off. Treating it as an approximation rather than an exact figure keeps the calculation honest.
The biggest source of error is that the calculation assumes the population is in Hardy-Weinberg equilibrium for the gene. If a population has substantial inbreeding or consanguinity, where relatives marry, the incidence of affected individuals rises above what the carrier frequency alone would predict, because related parents are more likely to share the same recessive allele. In such populations, working backward from the elevated disease incidence can overestimate the true carrier frequency. Population stratification, where a population is really a mix of subgroups with different allele frequencies, can distort the estimate in similar ways. The neat 2pq relationship assumes a single, randomly mating population.
Another limitation concerns conditions caused by many different mutations in the same gene. For a disorder like cystic fibrosis, hundreds of distinct mutations can each cause the disease, so the q in the equation really represents the combined frequency of all disease-causing variants. This works for estimating overall carrier frequency, but it complicates carrier testing, since a test must check for many specific mutations and may miss rare ones. The Hardy-Weinberg estimate gives a useful population-level number, but individual carrier testing is more precise for a specific person. These caveats do not undermine the method; they simply mean the carrier frequency is a well-grounded estimate that works best for large, randomly mating populations and should be interpreted with care where those conditions break down.
When the Gene Has Several Common Variants
Most carrier-frequency teaching uses a simple two-allele model, but some genes have more than one common variant, which slightly changes how you think about carriers. Understanding this extends the concept to more realistic situations.
When a gene has a single recessive disease allele, the carrier frequency is the straightforward 2pq. But when several different recessive alleles can each cause a condition, an individual can be affected by carrying any two disease alleles, which need not be identical. Such a person is called a compound heterozygote, carrying two different disease-causing variants rather than two copies of the same one. For population calculations, q is treated as the total frequency of all disease alleles combined, and the affected frequency q² then includes both true homozygotes and compound heterozygotes.
This generalization matters for real disorders, where the disease incidence reflects every combination of disease alleles, not just one. The good news is that the Hardy-Weinberg framework still works: by pooling all disease-causing variants into a single q, you can estimate the overall carrier frequency just as before. The complication is mainly practical, affecting how carrier tests are designed rather than how the population math is done. For most teaching and screening purposes, treating the disease allele as a single combined q gives an accurate carrier frequency, which is why the simple 2pq approach remains the standard starting point even for genetically complex conditions.
Why Carrier Frequency Matters in Genetic Counseling
Carrier frequency is not an academic exercise; it is central to genetic counseling and reproductive health decisions. Knowing how common carriers are lets counselors estimate the risk that a couple will have an affected child, which is often the question families most want answered.
The logic connects carrier frequency to offspring risk. If carriers occur at a known frequency in a population, then the chance that a random person is a carrier is that frequency. For two random partners, the chance both are carriers is the carrier frequency multiplied by itself, and if both are carriers, a Punnett square shows a 1 in 4 chance for each child to be affected. Combining these gives the population-level risk for a couple with no family history. This is exactly how carrier screening programs estimate and communicate risk, and the carrier probability calculator handles these combined calculations for specific scenarios.
Real genetic counseling layers additional information on top of the population estimate. Family history changes the numbers significantly: if a couple already has an affected child, or has affected relatives, their carrier risk is much higher than the population baseline, and the calculation adjusts accordingly. Carrier testing can also confirm or rule out carrier status directly, replacing the population estimate with certainty for those individuals. The Hardy-Weinberg carrier frequency provides the starting baseline, the default risk before any family-specific information is added, which makes it the foundation that personalized counseling builds upon.
Frequently Asked Questions
How do you calculate carrier frequency with Hardy-Weinberg?
Carrier frequency is 2pq. Start from the disease incidence, which equals q², take its square root to find q, use p + q = 1 to find p, then multiply 2 times p times q. The result is the proportion of the population that carries one copy of the recessive allele.
Why are there more carriers than affected people?
Because carrier frequency 2pq is much larger than disease incidence q² when the allele is rare. Most copies of a rare recessive allele are hidden in healthy heterozygous carriers rather than expressed in affected homozygotes, so carriers greatly outnumber affected individuals.
What is the carrier frequency for cystic fibrosis?
In northern European populations, cystic fibrosis affects about 1 in 2,500 people, giving a carrier frequency of roughly 1 in 25. So while the disease is relatively uncommon, about one in twenty-five people carries the allele without showing any symptoms.
Is there a shortcut for carrier frequency?
Yes, for rare alleles. Since p is close to 1, the carrier frequency 2pq is approximately 2q, which is roughly twice the square root of the disease incidence. Take the square root of the disease frequency and double it for a quick estimate.
Where the 2pq Step Leads
Carrier frequency comes down to a single term, 2pq, calculated from the disease incidence. Start with q² as the disease frequency, square-root it to find q, find p from p + q = 1, then multiply 2pq to get the carriers. The defining lesson is that carriers vastly outnumber affected individuals for rare conditions, because most copies of a recessive allele hide in healthy heterozygotes, which is also why such alleles persist over generations.
This calculation is where Hardy-Weinberg becomes genuinely useful in the real world, underpinning genetic counseling, carrier screening, and public health planning. You can run any carrier-frequency calculation with the Hardy-Weinberg allele frequency calculator, which finds q, p, and 2pq from a disease incidence instantly. For an authoritative walkthrough of these clinical calculations, this genetic risk resource from the University of Kansas Medical Center is a reliable reference.
This article explains carrier frequency for educational purposes. If you have personal concerns about carrier status or inherited conditions in your family, a licensed genetic counselor or physician can provide guidance tailored to your situation and is the right source for decisions about testing.